

K-Christian's Fletcher Brought Calm, Kindness
October 13, 2020
By Geoff Kimmerly
Second Half editor
The calm in a storm. The rock, no matter how bad things would get.
That’s how longtime athletic administrator Karen Leinaar described Ken Fletcher, who served as director of Kalamazoo Christian’s athletic department for three decades and was among those from the Kalamazoo Valley Association who mentored Leinaar when she served at Delton Kellogg during the 1980s and 90s.
Fletcher died Sept. 25 at age 77.
He had spent 40 years total in education, also as a teacher and coach, before retiring in 2006.
“Anytime we had an issue in the league, he was the calming voice, he was the voice or reason,” said Leinaar, now athletic director at Bear Lake and executive director of the Michigan Interscholastic Athletic Administrators Association. “Being a mathematician, he was a very logical thinker – but he had the compassion of a priest.
“You never saw Ken disheveled. You never saw Ken frustrated. He always had a smile and kind word for everybody – it didn’t matter the color of their uniform or if it was an official or spectator.”
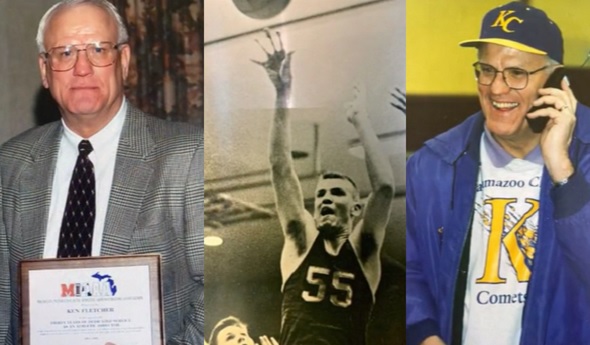
Fletcher had graduated from Kalamazoo Christian in 1961 and was part of the boys basketball team that won the Class C championship in 1959. He went on to Calvin College (now Calvin University), where he majored in mathematics and earned a degree in education, and also continued his basketball and baseball careers. He later received master’s degrees in in athletic administration from University of Michigan and mathematics from Western Michigan University.
Kalamazoo Christian’s boys basketball team also won Class C championships in 1983 and 2001 during Fletcher’s AD tenure. But Leinaar noted that Fletcher was a great advocate as well for the school’s girls programs, which often were more frequently successful – the softball team, for example, won six MHSAA Finals titles over seven seasons from 1996-2002. “He just loved kids,” she added.
Fletcher was named his region’s Athletic Director of the Year by the MIAAA in 1989.
He is survived in part by his wife of 56 years, Judy, three children and 14 grand- and great-grandchildren. Click to view Fletcher’s full obituary.
PHOTOS collected by the Fletcher family.

Schools Continue to Manage the Heat
July 16, 2015
By Rob Kaminski
MHSAA benchmarks editor
It certainly was not the MHSAA’s intent to spur the most historically frigid back-to-back winters the state has seen. Nor did the Association wish for one of the mildest summers in recent memory during 2014.
Seemingly, it’s just Mother Nature’s way of reading into MHSAA efforts for managing heat and humidity and acclimatizing student-athletes for warm-weather activities.
Since guidelines were put in place (recommended for regular-season sessions and required for postseason tournaments) before the 2013-14 school year, there have been relatively few days during which psychrometers have had to be implemented.
“The key is, we’ve got plans in place for when the climate returns to normal trends for return-to-school practices and contests in August and September, as well as early June events,” said MHSAA Executive Director Jack Roberts. “It is a bit ironic that there have been relatively few days since the guidelines were established that they’ve actually come into play.”
In a nutshell, the guidelines provide instruction for four ranges of heat index: below 95 degrees; 95-99 degrees; 99-104 degrees, and heat indexes above 104 degrees, with increasing precautions in place as heat indexes rise. An index above 104 calls for all activity to cease.
Certified athletic trainers Gretchen Mohney and James Lioy agree that recent requirements in heat and hydration guidelines are a step in the right direction and encourage that – when possible – an athletic trainer oversee the implementation. Simply taking a reading from just outside the AD’s office or at home does not simulate on-site conditions.
“This doesn’t take into account the radiant heat at the site, which can drastically affect the conditions that athlete plays in. It is essential that all parties involved in making decisions to play collaborate with one another,” Mohney said.
Heat-related deaths in athletics rank only behind cardiac disorders and head and neck injuries, but such fatalities might lead the way in frustration for families and communities of the victims. The reason? Heat-related illness is totally preventable.
Another source of mild frustration is the lack of recording within the state for those practice and game situations which warrant heat protocols.
When the Representative Council was formulating the Heat and Humidity Policy, it was also mindful of ways in which the MHSAA could assist schools in putting the plan into practice. Coaches, athletic directors and trainers needed a method to record information for athletic directors to view and for the MHSAA to track. The MHSAA developed interactive web pages on MHSAA.com which allow registered personnel to record weather conditions as practices and contests are taking place, using psychrometers.
Additionally, discounted Heat and Humidity Monitors and Precision Heat Index Instruments are offered to schools through a partnership between the MHSAA and School Health.
Yet, since the availability of such tools came to fruition two years back, fewer than 1,000 entries have been recorded, and many are multiple entries from the same schools.
Of the 772 entries, only 15 took place when the heat index was in excess of 104, while just 21 indicated an index of greater than 100. Cooler temperatures could be playing a factor in the overall number of participation, particularly in the northern areas of the state.
Nearly all of the responses came during fall practices, with a few isolated cases coming during the spring.
As Mohney pointed out, all resources must be properly used in concert with one another to achieve desired results.
Reminders of the tools available to schools are disseminated throughout the state each summer.